Our editors pick the products and services we write about. When you buy through our links, we may get a commission. Learn more.
5 Differences Between CBD and THC

In This Article
What is CBD?
What is THC?
CBD vs. THC: Key differences
Chemical structure
Psychoactive Properties of CBD vs. THC
Legality of CBD vs. THC
Medical Benefits of Cannabinoids
CBD vs THC for Chronic Pain
FDA-Approved Uses
Safety and Side Effects of CBD and THC
Recreational effects of CBD vs. THC
Product Forms
Consumption Methods
Drug Testing for Cannabinoids
Final thoughts
References
What is CBD?
Cannabidiol (CBD) is a non-intoxicating cannabinoid, which means it won’t cause the mind-altering effects associated with cannabis. It’s usually derived from hemp, a variety of cannabis with low THC levels (0.3% or less).
In regular cannabis, CBD is the second most prevalent cannabinoid. CBD has rapidly grown in popularity in the past several years as a natural option for relieving a wide variety of symptoms and conditions.
What is THC?

Tetrahydrocannabinol (THC) is the most abundant cannabinoid in marijuana, the term for cannabis plants that can get you high. By definition, marijuana contains over 0.3% THC, with some strains reaching concentrations as high as 30%.
As the main psychoactive component of cannabis, THC is largely responsible for the cannabis high. However, like CBD, it also has many potential health benefits.
CBD vs. THC: Key differences

CBD and THC do have a lot in common. They’re both phytocannabinoids (plant-derived cannabinoids) found in the cannabis plant, which are different from the endocannabinoids naturally produced by our bodies. Many of their effects are also similar.
Having said that, CBD and THC differ in some key ways, such as their chemical structure, psychoactive properties, legal status, medical benefits, side effects, product forms, and more.
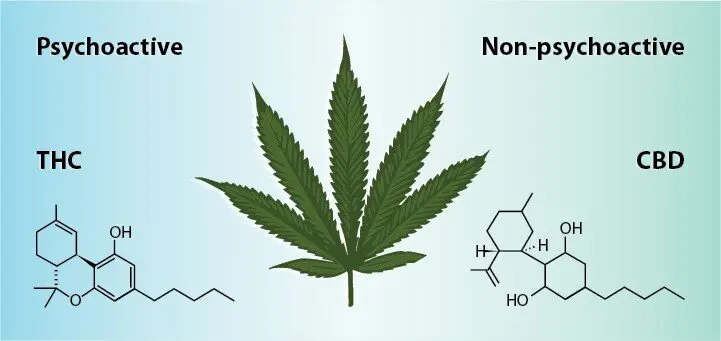
Chemical structure
Since CBD and THC are similar in structure to endocannabinoids, they can mimic their effects, interacting with cannabinoid receptors and other parts of the body’s endocannabinoid system (ECS).
In fact, CBD and THC have the same molecular formula. However, the way their atoms are arranged is different. This is arguably the biggest difference between CBD and THC as it’s responsible for their distinct effects.
Psychoactive Properties of CBD vs. THC

Legality of CBD vs. THC
Legality is another important factor when comparing CBD vs. THC.
Hemp-derived CBD is federally legal thanks to the 2018 Farm Bill, which legalized hemp and once again turned it into an agricultural commodity after decades of prohibition.
Under this law, hemp and any CBD products derived from it are legal as long as they contain no more than 0.3% THC by weight.
Every state also has its own laws relating to hemp and CBD. Although most align with federal policy, some are more restrictive and it’s best to research the laws of the particular state you’re interested in.
On the other hand, marijuana is a Schedule I controlled substance. This means both THC and CBD sourced from marijuana are illegal, except for the growing number of states that allow for recreational marijuana use, such as Colorado and California.
Additionally, medical marijuana is legal in most states.
Keep in mind that cannabis laws are always changing and it’s likely to become legal in more states as time goes on.
Medical Benefits of Cannabinoids

Research has shown that CBD and THC have a wide range of potential health benefits, many of which are similar. For example, they can both relieve pain, inflammation, and nausea.
However, some of their effects are distinct. More importantly, CBD is preferred by people looking for intoxication-free relief.
Multiple human studies suggest that CBD may help with:
- Seizures
- Psychosis
- Anxiety disorders
There’s also weaker evidence that CBD could be beneficial for:
- Drug addiction
- Chronic pain
- Inflammatory bowel disease
- Type-1 diabetes and diabetic complications
- Skin conditions such as acne and eczema
- Neurodegenerative disorders such as Alzheimer’s disease
- Inflammatory diseases
- Cardiovascular diseases
- Arthritis
- Depression
- Multiple sclerosis
- Cancer
- Nausea
- Insomnia and other sleep disorders
On its own or as part of whole-plant cannabis, there’s strong evidence that THC may help with:
- Chronic pain
- Nausea
- Sleep problems associated with chronic pain and other issues
- Multiple sclerosis
There’s also weaker evidence that it may be helpful for:
- Stimulating appetite
- Tourette syndrome
- Posttraumatic stress disorder (PTSD)
- Glaucoma
- Cancer
- Headaches and migraines
- Skin conditions
- Arthritis
The level of evidence for these potential benefits of CBD and THC varies greatly, with some supported by high-quality clinical trials, and others only having been tested in petri-dish or animal studies.
Another key point is that while both CBD and THC can lower anxiety, THC seems to have a biphasic effect, which means that only low doses can provide relief whereas higher ones make anxiety worse.
Meanwhile, CBD is so promising that researchers believe it could help with a wide range of anxiety disorders.
CBD vs THC for Chronic Pain
Chronic pain relief is the most common reason people turn to CBD and THC-containing products. However, there’s some evidence that THC may have stronger analgesic (pain-relieving) effects.
More importantly, research suggests that CBD and THC work best as part of whole-plant cannabis preparations that contain the full range of cannabis cannabinoids, terpenes, flavonoids, and other active compounds.
FDA-Approved Uses
CBD, THC, and whole-plant cannabis are not currently approved for any medical condition.
However, the CBD-based pharmaceutical drug Epidiolex is FDA-approved for alleviating rare types of treatment-resistant epilepsy: Lennox-Gastaut syndrome (LGS), Dravet syndrome, and tuberous sclerosis complex (TSC).
Meanwhile, the THC-based drugs Marinol (dronabinol), Syndros (dronabinol), and Cesamet (nabilone) are approved for treating low appetite and weight loss associated with HIV/AIDS, and chemotherapy-related nausea and vomiting.
These drugs are only available via prescription.
Safety and Side Effects of CBD and THC
CBD and THC are considered relatively safe compounds. You’d need to use large doses to experience significant side effects, especially with CBD.
The most common side effects of CBD are tiredness, sleepiness, dry mouth, diarrhea, and changes in appetite.
However, these side effects are mostly minor and were only found in studies using large oral doses of pure CBD.
Even studies using daily doses as high as 1500 mg, which is much higher than those used by most people, found that CBD is tolerated well.
Additionally, the World Health Organization concluded in its 2018 report that “CBD is generally well tolerated with a good safety profile.”
THC can also cause tiredness, sleepiness, and dry mouth, as well as red eyes and increased heart rate. However, it’s better known for its psychoactive side effects, such as anxiety, paranoia, and impaired memory and concentration.
There’s also some concern that heavy, long-term THC use may increase the risk of psychiatric disorders such as schizophrenia but the evidence is inconclusive.
Lastly, both CBD and THC can potentially interact with prescription medications. However, these effects seem to require large doses and are not well-studied in humans. Nonetheless, it’s best to talk to your doctor before using CBD, THC, or any other cannabis product.
Recreational effects of CBD vs. THC
Many people use THC-rich cannabis because it can get you high, producing euphoria and other mind-altering effects.
In contrast, CBD isn’t often used recreationally since it doesn’t cause intoxication and appears to reduce the psychoactive effects of THC. This may explain why cannabis strains high in CBD are less intoxicating.
Product Forms
THC is most commonly used in the form of dried marijuana. As we noted above, there are also several synthetic, THC-based pharmaceutical drugs used for specific medical issues.
CBD is also used as part of whole-plant marijuana because it’s usually the second-most common cannabinoid in the plant after THC. Similarly, the pharmaceutical CBD drug Epidiolex is used for treating severe types of childhood epilepsy.
However, CBD is best known for coming in the form of full-spectrum CBD oil and other hemp-derived wellness products.
Both CBD and THC are also used in capsules, edibles, tinctures, vape products, concentrates, topical preparations, and other products.
Consumption Methods
THC and CBD can be consumed in a wide variety of ways. The four main options are:
- Inhalation: absorption through the lungs by smoking or vaping
- Oral: taking edibles, capsules, beverages, and other ingestible products by mouth
- Sublingual: absorbing cannabinoid-rich oil, tinctures, or sprays through the blood vessels under the tongue
- Topical: applying cannabinoids directly to the skin
Having said that, smoking cannabis is the most popular method of administering THC.
CBD is most commonly taken as sublingual CBD oil, although capsules, gummies, and other products are also used.
Drug Testing for Cannabinoids

Cannabis drug tests look for the metabolites of THC, which means that using marijuana and other THC-rich products will likely result in a positive test.
CBD itself won’t show up on a drug test. However, it’s possible to test positive when you use full-spectrum CBD products because they can contain up to 0.3% THC.
Final thoughts
Although similar in some ways, CBD and THC also have many key differences.
They both have a long list of potential health benefits that may help with a wide variety of conditions and symptoms. However, more research is needed to substantiate and fully understand their effects.
It’s also important to note that CBD and THC are best used together, especially in combination with other cannabinoids, terpenes, and flavonoids naturally present in cannabis.
Research has shown that these compounds work in synergy, which is commonly referred to as the entourage effect.
References
- Maccarrone, M. (2020). Phytocannabinoids and endocannabinoids: different in nature. Rendiconti Lincei. Scienze Fisiche e Naturali, 31(4), 931-938.
- Piomelli, D., & Russo, E. B. (2016). The Cannabis sativa versus Cannabis indica debate: an interview with Ethan Russo, MD. Cannabis and cannabinoid research, 1(1), 44-46.
- Mackie, K. (2006). Mechanisms of CB1 receptor signaling: endocannabinoid modulation of synaptic strength. International journal of obesity, 30(1), S19-S23.
- Chung, H., Fierro, A., & Pessoa-Mahana, C. D. (2019). Cannabidiol binding and negative allosteric modulation at the cannabinoid type 1 receptor in the presence of delta-9-tetrahydrocannabinol: An In Silico study. PloS one, 14(7), e0220025.
- Mlost, J., Bryk, M., & Starowicz, K. (2020). Cannabidiol for Pain Treatment: Focus on Pharmacology and Mechanism of Action. International journal of molecular sciences, 21(22), 8870.
- Iffland, K., & Grotenhermen, F. (2017). An update on safety and side effects of cannabidiol: a review of clinical data and relevant animal studies. Cannabis and cannabinoid research, 2(1), 139-154.
- Bergamaschi, M. M., Queiroz, R. H., & Zuardi, A. W. en Crippa, JA (2011). Safety and Side Effects of Cannabidiol, a Cannabis sativa Constituent. Current Drug Safety, 6(4), 237-249.
- https://www.who.int/publications/m/item/cannabidiol
- NIDA. 2021, April 13. Is there a link between marijuana use and psychiatric disorders?. Retrieved from https://www.drugabuse.gov/publications/research-reports/marijuana/there-link-between-marijuana-use-psychiatric-disorders on 2021, June 7
- Antoniou, T., Bodkin, J., & Ho, J. M. W. (2020). Drug interactions with cannabinoids. CMAJ, 192(9), E206-E206.
- Huestis, M. A., Solimini, R., Pichini, S., Pacifici, R., Carlier, J., & Busardò, F. P. (2019). Cannabidiol adverse effects and toxicity. Current neuropharmacology, 17(10), 974-989.
- Pisanti, S., Malfitano, A. M., Ciaglia, E., Lamberti, A., Ranieri, R., Cuomo, G., … & Bifulco, M. (2017). Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacology & therapeutics, 175, 133-150.
- Davies, C., & Bhattacharyya, S. (2019). Cannabidiol as a potential treatment for psychosis. Therapeutic advances in psychopharmacology, 9, 2045125319881916.
- Prud’homme, M., Cata, R., & Jutras-Aswad, D. (2015). Cannabidiol as an intervention for addictive behaviors: a systematic review of the evidence. Substance abuse: research and treatment, 9, SART-S25081.
- Irving, P. M., Iqbal, T., Nwokolo, C., Subramanian, S., Bloom, S., Prasad, N., … & Wright, S. (2018). A randomized, double-blind, placebo-controlled, parallel-group, pilot study of cannabidiol-rich botanical extract in the symptomatic treatment of ulcerative colitis. Inflammatory bowel diseases, 24(4), 714-724.
- Weiss, L., Zeira, M., Reich, S., Har-Noy, M., Mechoulam, R., Slavin, S., & Gallily, R. (2006). Cannabidiol lowers incidence of diabetes in non-obese diabetic mice. Autoimmunity, 39(2), 143-151.
- Baswan, S. M., Klosner, A. E., Glynn, K., Rajgopal, A., Malik, K., Yim, S., & Stern, N. (2020). Therapeutic Potential of Cannabidiol (CBD) for Skin Health and Disorders. Clinical, cosmetic and investigational dermatology, 13, 927.
- Babson, K. A., Sottile, J., & Morabito, D. (2017). Cannabis, cannabinoids, and sleep: a review of the literature. Current psychiatry reports, 19(4), 1-12.
- Abrams, D. I. (2018). The therapeutic effects of Cannabis and cannabinoids: An update from the National Academies of Sciences, Engineering and Medicine report. European journal of internal medicine, 49, 7-11.
- Novack, G. D. (2016). Cannabinoids for treatment of glaucoma. Current opinion in ophthalmology, 27(2), 146-150.
- Dariš, B., Verboten, M. T., Knez, Ž., & Ferk, P. (2019). Cannabinoids in cancer treatment: Therapeutic potential and legislation. Bosnian journal of basic medical sciences, 19(1), 14.
- Dariš, B., Verboten, M. T., Knez, Ž., & Ferk, P. (2019). Cannabinoids in cancer treatment: Therapeutic potential and legislation. Bosnian journal of basic medical sciences, 19(1), 14.
- Lochte, B. C., Beletsky, A., Samuel, N. K., & Grant, I. (2017). The use of cannabis for headache disorders. Cannabis and cannabinoid research, 2(1), 61-71.
- Sheriff, T., Lin, M. J., Dubin, D., & Khorasani, H. (2020). The potential role of cannabinoids in dermatology. Journal of Dermatological Treatment, 31(8), 839-845.
- Lowin, T., Schneider, M., & Pongratz, G. (2019). Joints for joints: cannabinoids in the treatment of rheumatoid arthritis. Current opinion in rheumatology, 31(3), 271-278.
- Bhattacharyya, S., Egerton, A., Kim, E., Rosso, L., Barros, D. R., Hammers, A., … & McGuire, P. (2017). Acute induction of anxiety in humans by delta-9-tetrahydrocannabinol related to amygdalar cannabinoid-1 (CB1) receptors. Scientific reports, 7(1), 1-15.
- Blessing, E. M., Steenkamp, M. M., Manzanares, J., & Marmar, C. R. (2015). Cannabidiol as a potential treatment for anxiety disorders. Neurotherapeutics, 12(4), 825-836.
- Corroon, J., & Phillips, J. A. (2018). A cross-sectional study of cannabidiol users. Cannabis and cannabinoid research, 3(1), 152-161.
- Mlost, J., Bryk, M., & Starowicz, K. (2020). Cannabidiol for Pain Treatment: Focus on Pharmacology and Mechanism of Action. International journal of molecular sciences, 21(22), 8870.
- Banerjee, S., & McCormack, S. (2019). Medical cannabis for the treatment of chronic pain: a review of clinical effectiveness and guidelines.
- https://www.fda.gov/news-events/public-health-focus/fda-and-cannabis-research-and-drug-approval-process
- Niesink, R. J., & van Laar, M. W. (2013). Does cannabidiol protect against adverse psychological effects of THC?. Frontiers in psychiatry, 4, 130.
- Russo, E. B. (2019). The case for the entourage effect and conventional breeding of clinical cannabis: no “strain,” no gain. Frontiers in plant science, 9, 1969.


In This Article